
Could a simple intervention like B vitamins improve ED? Multiple human studies suggest they might
By far, the most common concern that comes up in discussions of male sexual health is erectile dysfunction. A large, multinational survey, published in 2004, found that erectile dysfunction (commonly referred to simply as ED) affects approximately 16% of males between the ages of 20 and 75,[1] and is increasingly common with age. But it is not a problem that just older men struggle with: a 2013 survey of men seeking treatment for ED at a urology center in Italy found that one in four were under the age of 40.[2] Additionally, a 2017 publication from a sexual health and endocrinology center reported that the percentage of men under 40 seeking care for ED had tripled from 2011 to 2014.[3] With the stress of the global pandemic, loss of jobs, social isolation, and frequent use of unhealthy coping behaviors, it is likely that beyond 2020 these statistics will continue to be increasingly bleak.
We’ve discussed many contributing factors to ED such as blood vessel dysfunction and inadequate nitric oxide (NO) levels, as well as nutritional factors that enhance the body’s endogenous NO production. We’ve discussed a standardized extract of maritime pine bark, which has clinical studies showing it supports healthy blood flow in blood vessels big and small, including multiple studies in men with ED. Herein, we direct our focus at the relationship between homocysteine levels and ED, as well as the improvements that have been seen clinically in various populations with ED and the simple intervention of B vitamins.
Homocysteine and erectile dysfunction
Elevated homocysteine levels are not only related to cardiovascular disease and Alzheimer’s dementia, they are common in erectile dysfunction.
Numerous studies have shown a relationship between homocysteine (HCY) elevation and erectile dysfunction. Elevated levels of HCY are associated with poor blood vessel dilation and dysfunction of the enzyme, nitric oxide synthase (NOS), which is responsible for the production of NO in blood vessels.[4],[5] Thus, we also see a relationship between elevated HCY and numerous conditions with vascular underpinnings including cardiovascular disease,[6] cognitive decline and Alzheimer’s disease,[7],[8] and chronic kidney disease.[9] High levels of HCY also create oxidative stress by a variety of mechanisms,[10],[11],[12] hence its broad relationship with many chronic conditions including depression and metabolic disease.[13],[14],[15],[16]
A 2018 systemic review and meta-analysis of nine studies including 1,320 individuals found that individuals having ED were approximately twice as likely to have elevated levels of HCY.[17] Elevated homocysteine has even been shown to be an independent risk factor for ED, particularly when it exceeds 12.65 micromole/L.[18] It has been reported that HCY levels above 14.3 micromole/L increases the risk of ED nearly fivefold in men with diabetes.[19]
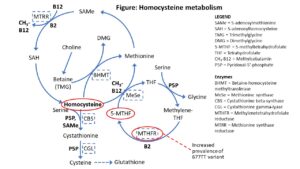
Proper metabolism of HCY requires numerous B vitamins and depends on the functionality of several enzymes (see Figure). Depletion of vitamin B12 or folate can have a major impact on HCY, increasing serum HCY by a factor of three to 20 times the upper normal limit.[20],[21] Low levels of folic acid have been shown in men with ED in multiple clinical studies.[22],[23] In addition to assessing B12 and folate levels, evaluation of serum methylmalonic acid (MMA) is important to distinguish between B12 and folate deficiencies. When MMA is not elevated but HCY is, a deficiency of folate is indicated, while if both are elevated, B12 is deficient.[24] However, if both are elevated, folate deficiency cannot be ruled out.
Treatment success with B vitamins
Folic acid has been shown in multiple clinical studies to improve erectile function in men with erectile dysfunction, including those already taking pharmaceutical medications for the condition.
Of these the B vitamins, folate rises to the top as an intervention for specifically addressing ED, with multiple clinical studies supporting its use. In men age 30 to 60 diagnosed with idiopathic vasculogenic erectile dysfunction, supplementation of 500 mcg of folic acid daily for three months significantly improved median ED scores on the commonly used ED scoring system, known as the International Index of Erectile Function (IIEF-5), from 6 to 14.[25] (For reference, on the IIEF-5 scoring system, a score of 6 is considered severe while 14 is in the mild to moderate range.) Parameters related to penile blood velocity also had highly significant improvements with the intervention. Although it was not a criterion for study inclusion, HCY levels were significantly higher at baseline in individuals diagnosed with ED (median of 2.84 micromole/L) compared to the control population, and were significantly reduced with the intervention to a median value of 0.19 micromole/L.
Folic acid has also been shown in a randomized, double-blind, placebo-controlled trial to improve ED scores in men with type 2 diabetes (T2D) when taken as an adjunctive treatment to a phosphodiesterase type 5 inhibitor (PDE5I). After being given folic acid at a dose of 5 mg/day for three months, an improvement in mean IIEF-5 scores from 11.65 to 16.80 was seen in those receiving both interventions, with final scores also being significantly better than those in the placebo group who received only the PDE5I medication.[26]
Finally, folic acid has been investigated in combination with inositol in patients with T2D. Inositol has been described as functionally being similar to B vitamins; but as the body produces it, it is not an essential dietary substance.[27] In the individuals with T2D, those receiving 400 mcg of folic acid in combination with 4 g of myoinositol daily for 12 weeks had significantly improved IIEF-5 scores from 12 to 20 while there were no significant improvements in the placebo group.[28]
Genetic variants related to folate methylation can be a factor in erectile dysfunction and supplementation with the active 5-MTHF form of folate may help circumvent these issues.
One reason why supplemental folate is a key factor for HCY metabolism relates to the enzyme methylenetetrahydrofolate reductase (MTHFR). MTHFR converts methylene-tetrahydrofolate to its more biologically active form, 5-methyltetrahydrofolate (5-MTHF, see Figure). A variant of the MTHFR enzyme, known as the 677TT polymorphism, has been shown to be more common in males with vasculogenic ED, particularly those who experience the problem at a young age.[29] With this genetic variant, homocysteine metabolism is compromised as the “gears” which must “rotate” to convert it to methionine in essence get stuck as there are inadequate amounts of 5-MTHF. One can push the system to cycle again by adding additional folate, ideally in the form of 5-MTHF to bypass the poorly functioning MTHFR enzyme.[30]
One study specifically considered the impact of folate and vitamin B6 supplementation on erectile function in individuals with the MTHFR 677TT and heterozygous 677CT variants who were non-responsive to PDE5I treatment.[31] After an initial intervention of treatment with the PDE5I for two months, a group of 18 individuals who were PDE5I non-responders were selected for the nutritional intervention which consisted of 15 mg of folic acid/day and 600 mg of pyridoxine hydrochloride (vitamin B6) twice weekly. At the re-evaluation point six weeks later, the combination of folic acid and vitamin B6 was found to improve IIEF-5 scores in 88.9% of the population, with almost half of them improving considerably.
Given the simplicity and essentiality of the B vitamins for so many aspects of health, they are worthy of consideration as a first-line nutritional intervention for numerous chronic issues. Mood disorders, cardiovascular and cognitive health, multiple sclerosis, attention deficit/hyperactivity disorder, and so much more may be benefitted by B vitamins as a therapy. B vitamins are typically well-tolerated, and best to be taken with a morning meal to avoid “B burps” or mild upper GI discomfort that can occur.
Click here to see References
Vitamin E and Immunity, Part 1 of 2
The aging immune system and vitamin E Many are familiar with the antioxidant principles of the vitamin E family, and their importance for the protection of cellular membranes and prevention of cholesterol oxidation.[1],[2] Vitamin E also is important for a healthy functioning immune system, and deficiency can play a role in declining immune function,…
Improving Erectile Health – Part 2 of 2
Nitric oxide support for sexual health In Part 1 of this series, we looked at the physiology of a type of erectile dysfunction (ED) known as endothelial ED and explained the importance of blood vessel health on male sexual function. This week, we will explore some natural strategies, that have good scientific evidence for…
The Immune-Boosting Power of Lactoferrin
Mother’s milk — for the rest of us The highest concentrations of lactoferrin are found in colostrum, the first form of milk produced by a mother’s mammary glands immediately after she gives birth. But don’t be fooled: lactoferrin supports the health and immune function of adults and babies alike. Lactoferrin has a myriad of…


